
My awesome sister, an anaesthetist, delivers epidurals for a job. So I asked her some questions about epidurals during labour and she kindly and candidly answered them. Shot sis!
“Holy shiiiiiit! I am pregnant. Not only am I pregnant, but I am in denial about having to get this rapidly expanding lime/lemon/grapefruit/pomelo out of somewhere that has previously only had one function!” And out of all the things to think about, having an epidural can be way way way down your list of important life decisions.
Epidurals….
Where to start?
There is a lot of propaganda out there about epidurals. A LOT. So my sister, who specialises in vaginas, wants me to write something about epidurals. Epidurals are used for all sorts of operations and anaesthetics, but mostly commonly for childbirth and this is how they are linked to her interest in vaginas. She has given me some questions that I will try to answer as medically as I can.
What are the common pain relief options I can request during labour?
Here is a good site from the NHS…
http://www.nhs.uk/conditions/pregnancy-and-baby/pages/pain-relief-labour.aspx
But essentially, the active pain relief options are
- Entonox (“laughing gas”)
- TENS machines – not shown to be effective
- Alternative methods eg accupuncture – not shown to be effective
- Opioid drugs – eg morphine, pethidine. Which drug is given will depend on your place of delivery. Pethidine has traditionally been used but due to safety concerns, there is a movement away from its use.
- Epidural
What is an epidural?
An epidural catheter is a long, small, thin tube that delivers local anaesthetic to your epidural space. The tip of the long catheter has a few holes that the local anaesthetic drugs come out from. The drugs are administered from the other end which is usually secured over your shoulder.
The aim of an epidural catheter is to allow you to deliver your baby (or babies!) while awake. You can have a low dose local anaesthetic epidural that aims to numb the pain but not your muscles and allows a otherwise normal vaginal delivery, or you can have a high dose that not only numbs the pain but usually numbs your muscle function and allows more invasive ways of delivering the baby (e.g. caesarean section).
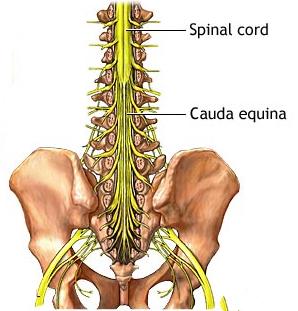
The epidural space is a space around the dura. The dura is the layer of tissue that encases your spinal cord and spinal fluid. This is an important difference as the epidural does not go into the space that holds your spinal cord. Occasionally (1 in 200 actually), the epidural can be accidentally placed a level too deep and in through the dura. There is an extra safety system in an epidural placed for labour in that the actual spinal cord finishes in most adults at a much higher level than where the epidural is going. So, while there are nerves lower down, there is no spinal cord in the area where we place these epidurals. (Myth number one busted: the epidural is NOT placed with a large needle straight into your spinal cord).
The spinal cord ends around the highest of the lumbar (lower back) vertebrae Image credit: https://www.studyblue.com/notes/note/n/spinal-cord/deck/4195980
An epidural works because your nerves come out from the dura and travel through the epidural space to get to your arm/leg/skin/uterus/vagina/etc. The local anaesthetic blocks the electrical signal travelling up (or down) the nerve and stops pain signals getting through.
What are the advantages of an epidural?
I think this might be time to bust myth number two. No one will force you to get an epidural. There can be times when medically your delivery team will suggest that the safest option may be to have an epidural, there may be a time when you want an epidural and there may be a time when you don’t. Whatever your choice, it is your choice and the anaesthetist needs your consent to put an epidural into you.
The RCOG (Royal College of Obstetricians & Gynaecologists) in the UK have some international guidelines that I think are important. Here are some of the pertinent points from RCOG, in respect to epidurals:
- The decision to have an epidural analgesia should lie with the woman, in consultation with her midwife or obstetrician.
- Women should also have available to them, good antenatal education to ensure they are informed about all methods of pain relief to allow them to make an informed choice about what they would like to use in labour.
- Pain during childbirth is very subjective and differs from woman-to-woman. Women should therefore be supported in their birth choice and should not be made to feel that their experience of childbirth is diminished if they decide to have an epidural analgesia.
So a common reason for an epidural is to ease or stop the pain of labour or of a caesarean section. If you were to have a caesarean section, there are thought to be advantages to both you and to your baby of being awake for the delivery.
There are times when it may be suggested by your obstetric team that the safest thing to do is to have an epidural. Some of the times this may happen are for multiple births, prolonged labour, the baby being in a breech position and certain medical conditions (e.g. certain types of heart disease). “Women with high blood pressure may also benefit from an epidural which, by relieving the pain, may make the blood pressure easier to control. Likewise, if a woman has a deep-rooted fear of childbirth, the use of pain relief will be welcome to her and may encourage her to deliver normally rather than asking for a caesarean section.” (That quotation bit is straight from the RCOG website).
What are the disadvantages of an epidural?
Well, luckily epidurals have been found to be safe. (Myth number three busted).
As with any medical intervention though, there are risks. Usually what happens is that, as a labouring woman, you are assessed then your consent is obtained then the epidural is placed and you have a nice (pain free) delivery. Occasionally things do not go this way and I have outlined some of the disadvantages below:
- An anaesthetist has to place the epidural. This isn’t really a disadvantage, but it does mean you have to be in a hospital if you want an epidural.
- They don’t always work as well as we want them to. This will happen to around 1 in 8 women. It means you may have a “patchy block”, a one sided epidural or one that doesn’t work at all. Sometimes we can fix this, sometimes we need to put a new epidural in and very occasionally we can’t fix things at all.
- A dural puncture: this is what I briefly touched on above. It is when the needle to place the catheter ends up one layer too deep. It is usually identified at the time, but not always. It happens around 1 in 200 times we place an epidural and can cause a terrible (but very distinctive) headache. The treatment of it can sometimes be another injection in your back a few days down the track.
- Drop in blood pressure. The midwife in the room with you will monitor your blood pressure as appropriate.
- Instrumental delivery: So myth number four – “If you have an epidural then you will end up with a caesarean” – is not true. Having an epidural does not increase your risk of caesarean. It does increase your risk of having an instrumental delivery (forceps or suction to get the baby out) however. Having an instrumental delivery increases your risk of pelvic floor damage.
This is not a complete list. There are serious risks with an epidural, but they are thankfully really, really rare. If you are worried about these then it is worth discussing this with an anaesthetist before you enter labour. Your LMC can always refer you to an antenatal anaesthetic clinic to discuss your concerns.
Will I have back-pain FOREVER after an epidural?
No.
Well, maybe. But not BECAUSE you had an epidural (myth number 5).
There are multiple studies from around the world that involve 1000s of women and show that you may have back pain after an epidural. But the rate of chronic back pain in women who have had children is the same whether you had an epidural or not. Therefore, back pain after epidural is most probably not from the epidural, but from the changes in your body from pregnancy and childbirth, postural issues, your type of work, poor core activation or anatomical issues. If you have back pain after an epidural, get checked by your doctor. Once cleared by your doctor, see a women’s health physio for back pain advice and exercises to recover after childbirth.
Did you have an epidural when you had your babies?
Do you know what? That is irrelevant. The decision to have an epidural is yours and yours alone. Having an epidural does not make you a failure, and not having one doesn’t either. At the end of the day, having a healthy baby and a healthy mum is what is important and in this case, the end justifies the means.
You may plan to have an epidural-free birth but your labour and your baby might not have got the memo. If you have any questions, then I suggest primarily addressing them with your LMC or obstetric team, and you can always be referred to an antenatal anaesthetic clinic for more information.
Kia Ora!
– the vagina physio
Image credit: http://anestesiadexeus.com/en/pacientes/paciente-embarazada-la-anestesia-en-el-parto/tecnicas-analgo-anestesicas/